Situation:
One of the 3 strategic pillars of this plan for the health and social care system is Reform – “a renewed and concerted focus on prevention”
Nutrition is a core prevention issue, not a “supportive” intervention.
Hospital malnutrition is strongly associated with increased length of stay and higher readmission rates. Impaired wound healing, a higher risk of falls, infections and complications, and greater morbidity and mortality. Research consistently demonstrates that malnourished patients require significantly more complex care and place increased demand on hospital resources, ultimately driving higher healthcare costs.
Failure to identify and address malnutrition increases pressure on acute services and undermines prevention agendas.
Given these consequences, it is essential to take a proactive approach to preventing hospital‑acquired malnutrition. This requires first identifying the system‑level barriers that limit effective nutritional care so that targeted, sustainable solutions can be developed and implemented across the organisation.
Overall Project Aim; How might we by April 2026, reduce in-hospital weight loss in patients on 3 acute medical wards with a MUST score ≥2 by 5%.
Task:
Observational work was undertaken during April and May 2025 to look at the snack provision offered to patients across a range of acute across wards in a district general hospital. When patients where asked ‘are you currently offered snacks between meals’ 57% responded as ‘yes’ however the offering was a hot drink and a biscuit. When asked ‘Do you feel like you have lost any weight while in hospital’, 50% felt they had with 21% unsure.
Staff feedback across these acute wards was also paramount to driving change improvement, when asked ‘how well do you think the current snack options meet the dietary needs of patients’, 0% responded as ‘very well’, 22% ‘not at all’, 29% ‘slightly’, 29% ‘moderately’ and only 20% felt the current snack options met patients’ dietary needs well. Key themes emerged from staff around the challenges with snack options available with variety being the mainstay.
Qualitative feedback was compelling, one of our long stay patients with dysphagia vocalised the essential need for change, ‘if I need to see another pot of yoghurt again’.
The observational work clearly demonstrated an immediate need for change, the snack provision was insufficient to meet the recommended 2xsnacks daily equating 300kcal, 7g protein as outlined in the British Dietetic Association ‘Nutrition and Hydration Digest’. Both patients and staff identified that current snack provision were insufficient in variety, nutritional value, and ability to meet specific dietary needs. These insights reinforce the importance of developing a more comprehensive, patient‑centred approach to between‑meal nutrition to help mitigate hospital‑acquired malnutrition.
Action:
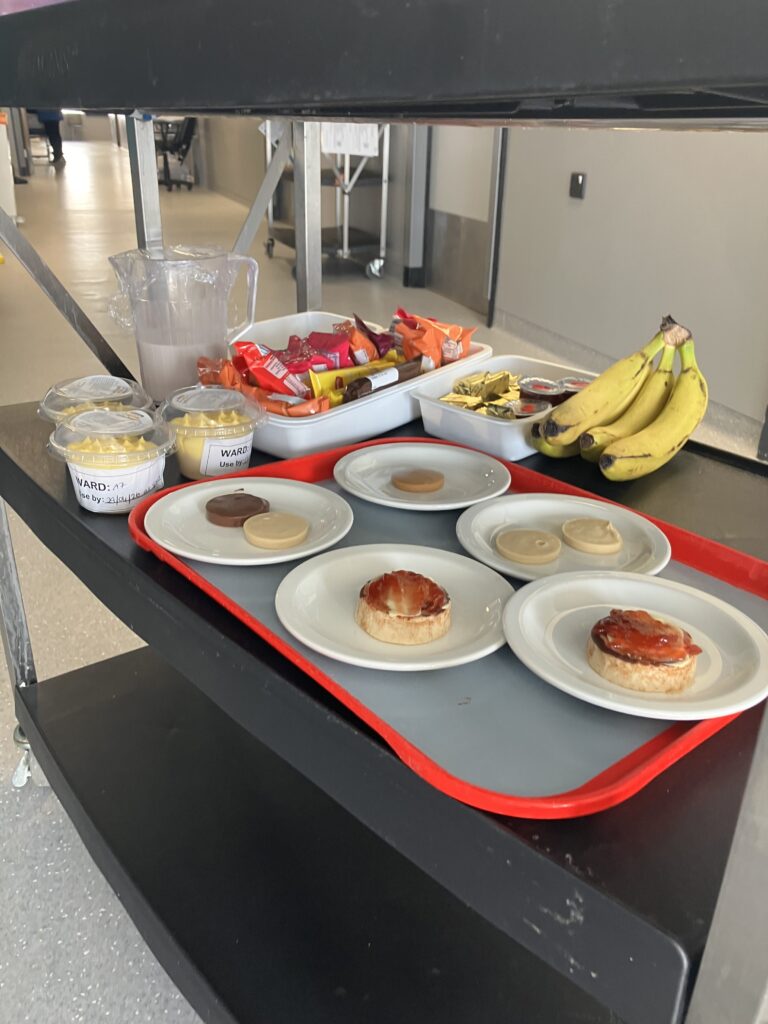
Improvement work commenced looking at the provision of snacks across different ward settings; care of the elderly, stroke and frailty in June 2025. Collective leadership was paramount to this work, identifying key roles and responsibilities to bring about sustainable change. Fundamental to this work was bringing together colleagues from across different divisions within the Trust, Nursing, Corporate Support Services, Dietetics, AHPs, Personal Public Involvement Team. Initial meetings were set up on each of the wards with ward managers, domestic and catering support service staff, dysphagia support team and myself as QI Lead for Dietetics. This approach was taken to really tailor the intervention to the needs of the patient population within each clinical area, allowing clear refinement of roles and responsibilities, what would work well within that area as well as identifying any areas of challenge that required further solutions-based focus. Exploring what was happening across the health service at a national level was also key to this improvement work in order to enhance both safety and quality. Regular meetings were held with the National Lead for Food within NHS England, benching marking and scoping both best practice and innovation happening within this area. Sustainability and waste management were other key areas to this work aligning with the HSC drive to net zero with an aim to reduce greenhouse gas emissions by 48% by 2030. Food items such as over-ripened bananas that would have been otherwise thrown away were incorporated into a home-made banana cake for patients. Other cake and scone mixture leftover from the production for public sale within Trust eateries was utilised and made into small home-made scones for patients. Scoping for pantry stores was also carried out to ascertain what we had within our current disposal that would enhance patient nutritional intake prior to the purchase of any new food items.
Change was embedded, snacks now available provide up to 358 kcal and 15.3 g protein per serving, representing a four‑fold increase in calories and a five‑fold increase in protein.
Qualitative feedback from our patients in 2025 highlighted the fundamental need for a review and expansion of snack options made available to those who have Dysphagia. In April 2026, our modified texture snack range was expanded following connections made at the Healthcare Caterers Association event. Patients on a puree texture diet now have twice as many choices. Significantly improving patient choice and nutritional intake, as the previous offering was largely limited to yoghurt and custard.
Full‑fat milk became the default across participating wards (124 kcal, 7 g protein per 200 ml), and breakfast porridge fortified with cream at ward level providing an additional 100 kcal/ serving.
The commencement of an in-house milkshake was taken forward initially in one care of the elderly ward, undertaken by nursing staff providing an additional 200 kcal and 9 g protein per 200 ml made through the use of simple store ingredients.
Other wards were also keen to embrace this change which presented complexities and challenges around equipment, staffing and waste. A system wide approach was undertaken to addressing these challenges, benefits to patient care were evident coupled with a willingness to improve nutritional care and so the catering team agreed to undertake this additional task allowing equity and consistency of this nourishing fluid for all wards involved in the intervention.
In addition to optimising nutritional intake, families have reported improved comfort and enjoyment for relatives at end of life, with one family reporting: ‘Mum really enjoyed the milkshake in her last few days of life.’
Result:
Data Quality
This Quality Improvement Initiative studies 194 Patients with a Malnutrition Score (MUST >2) between January – December 2025.
Patient Outcomes
Weight Maintenance improved in 2 out of 3 wards from 31% of patients on one ward maintaining their weight pre intervention → 40% maintaining weight post intervention and the other ward seeing an increase in those maintaining weight pre – post intervention from 11% → 28%.
Significant weight gain was also noted, 10% increase in 2 out of 3 wards pre -intervention on ward had 17% of patients gain weight with an average weight gain 4.9kg → post intervention this increased to 27% of patients with an average weight gain 5.2kg. Similarly, the second ward pre intervention had 24% of patients gain weight with an average weight gain 3.5kg → increasing to 34% gaining weight during admission with an average weight gain 4.5kg.
Length of Stay Reduced
Ward 1 average length of stay pre intervention 23.5 days → 17.7 days (post intervention) seeing an overall reduction of 5.8 bed day equating to £2,227.20/ patient.
Ward 2 average length of stay pre intervention 36.7 days → 32.3 days (post intervention) seeing an overall reduction of 4.4 bed days, £1689.60/ patient.
Ward 3 average length of stay pre intervention 40.8 days → 32.8 days seeing an overall reduction of 8 bed days, £3,072/ patient.
The need for oral nutritional supplement support was also reduced across all 3 intervention wards equating to a cost savings of £18,898.88.
This work has demonstrated improved patient flow and generated systemic cost savings and benefits for patient care.
Service Users and their families have also reported greater satisfaction and quality of nutritional care and patient experience is now more equitable for those with eating, drinking and swallowing problems.
other comments:
This project work has continued to develop and enhance, w/c 20th April has seen the expansion of snack options for those patients with a swallowing problem, to now include a puree scone, puree biscuits along with different flavours of mousse and a coffee dessert option. Preliminary qualitative feedback from colleagues across nursing, catering support and AHP services has been extremely positive. Supporting the roll out on clinical wards has also allowed for patient and carer feedback, improvement in patient experience and quality has been evident within the infancy of this next phase within the ‘Food is Medicine’ project.